
Alexithymia and Menopause: Why You Feel Nothing
What follows is a composite story drawn from real clinical patterns I see in my practice. Identifying details have been changed to protect patient privacy in accordance with HIPAA.
The Brain Behind Alexithymia: Why Menopause Makes It Harder to Feel What You're Feeling
She sat in her car long after pulling into the driveway.
The grocery bags in the back seat were starting to sweat in the Houston heat, but she didn't move. She was scrolling through an old playlist — songs that used to make her sing at the top of her lungs. She let them play one after another, waiting for that little spark she used to feel in her chest.
It never came.
The music was just sound. The light through the windshield was warm and golden, but it slid past her like water off glass. She wasn't sad. She wasn't happy. She wasn't anything.
When we finally spoke, she told me: "It's like my body forgot how to react. I can see things, hear things — but they don't get in anymore."
You follow what I'm saying? What she was describing has a name in the research — and perimenopause may have turned the volume on it all the way up.
This Has a Name — and It's Not "Just Stress"
What she was describing has a clinical name: alexithymia — the difficulty identifying, naming, and connecting with your own emotions. Not the absence of feeling. The absence of access to what you're feeling.
It's more common than most people realize, especially in women who are neurodivergent, who carry trauma history, or who have spent decades running at high function while pushing everything internal to the side. And when perimenopause hits — when estrogen starts its unpredictable fluctuation — a system that was already working differently under the surface suddenly gets a whole lot louder about it.
Most women don't get told this is even possible. They get told they're stressed. Or they're told to practice self-care. Or they get a depression screening that comes back inconclusive because what they're experiencing doesn't fit neatly into the diagnostic boxes that were built for a different presentation entirely.
Listen. The brain doesn't fail at this. What the research suggests is that it may be trying to translate through a system that lost one of its primary support structures. That's a different conversation than the one most clinicians are having.

What the Research Shows About Your Brain and Emotional Processing
Two structures are central to how the brain senses and processes emotional experience.
The insula is an interoception hub — it's involved in sensing what's happening inside the body. Heartbeat, tension in the chest, a warmth spreading through the stomach, the subtle flutter that used to signal excitement. Research suggests the insula is involved in taking that raw body data and translating it into something the mind can recognize and name.
The amygdala is sometimes described as an emotional smoke alarm — involved in detecting and prioritizing emotional signals, flagging what matters, and connecting past experience to present moment.
Both of these structures have estrogen receptors. When estrogen starts to fluctuate — and in perimenopause it doesn't just decline, it swings — the sensitivity and connectivity of these regions shifts. Research published in the Journal of Affective Disorders showed directly that estradiol modulates connectivity between the insula and other emotion-processing brain regions. When estradiol shifts, so does the bridge. (DOI: 10.1016/j.jad.2024.11.068)
For some women, that shift may mean the volume knob on emotional awareness gets turned way down. The sensations may still be happening. The translation just isn't completing.
Add a history of chronic stress or trauma to that picture — and a nervous system that has already learned to create distance from emotional cues as a survival strategy may have even less hormonal support helping it stay connected to itself.
That's not weakness. That's a nervous system that learned what it needed to learn to survive — in conditions that may now be making emotional access harder than ever.
The "Out of Body" Feeling Is Real
Many women describe this phase of perimenopause as feeling like they're watching their life instead of living it. Cooking dinner without tasting it. Listening to someone's story without feeling the response you know you should feel. Hearing music that used to move you now land as just sound.
It's not laziness. It's not losing your edge. It's not that you don't care.
What the research suggests is that your nervous system may be trying to process emotional experience through a translation system that is under hormonal stress — in many cases for the first time in your awareness, because a buffer that was compensating for a lifetime of different wiring may have just been significantly reduced.
The brain is working harder. Research following women across the menopause transition found that the brain actually recruits more cognitive regions to process emotion during this period — not fewer. It's expanding its effort, not retreating. (DOI: 10.1016/j.psyneuen.2016.08.026)
More effort. Less result. That's exhausting in a way that has nothing to do with attitude and everything to do with biology.
What Actually Helps — and Why Most Advice Misses It
The standard advice — name your emotions, journal your feelings, rate your mood on a scale of one to ten — is built on the assumption that you have direct verbal access to your emotional experience. For women with alexithymia, that assumption is exactly the problem. You're being asked to do in words what your brain can't yet do in words.
What works is starting before the words. Body data first. Translation second.
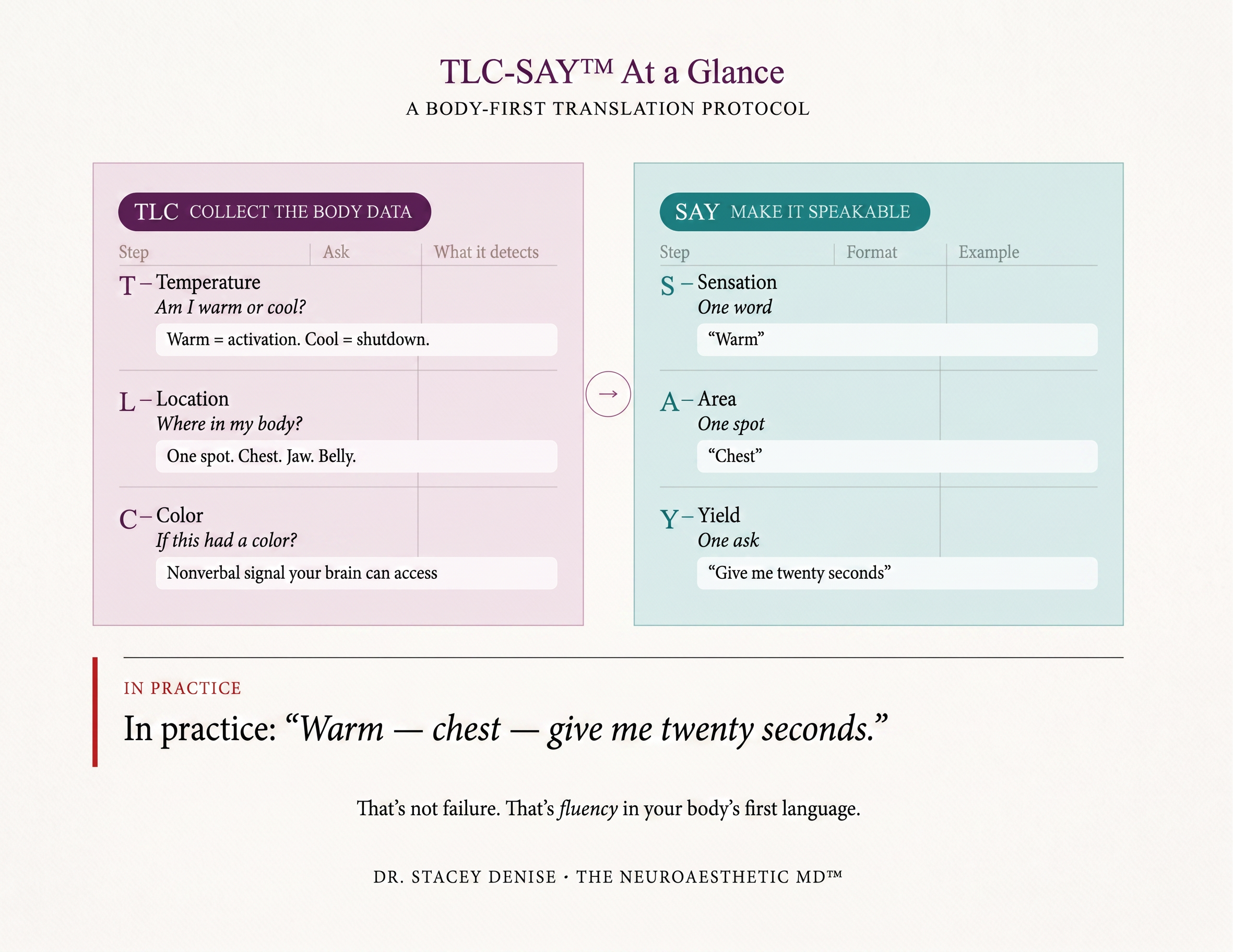
I developed a framework for exactly this — called TLC-SAY™ — because nothing that existed was built for a nervous system wired the way mine is. It starts where the brain can actually access the signal: temperature, location, and color. Not "what am I feeling." Just: am I warm or cool right now? Where in my body do I notice something? If this had a color, what would it be?
Then SAY converts that into the minimum language needed to communicate: one sensation word, one body location, one ask. "Warm — chest — give me twenty seconds." That's not failure. That's fluency in your body's actual first language.
The brain is not fixed in a flat state. The insula responds to training. Research by Dr. Kelly Mahler — one of the world's foremost experts on interoception, who I've spoken with directly — shows that interoception-based intervention measurably improves both interoceptive awareness and emotional regulation. (DOI: 10.1080/07380577.2024.2313527) The brain can rebuild the bridge. It just needs to be approached in the right sequence.
That's exactly what we do inside the Color Reset Series — through color, ritual, and body-first practices that work with the nervous system you actually have rather than the one the standard wellness industry assumes you have.
Her flat moments began to shift. Not overnight. Not dramatically. One day she called to tell me she was cooking dinner and found herself humming along to a song. "It wasn't even my favorite," she said. "But I felt it. I could feel me again."
You don't have to stay on the other side of the glass.
The Neurodivergent Consideration
If you're autistic or ADHD — or if you suspect you might be — this picture is more layered. Research shows alexithymia occurs in roughly 50% of autistic people compared to under 5% of neurotypical people. (DOI: 10.1016/j.eurpsy.2018.09.004) And critically: alexithymia is not the same as autism. They co-occur. But the emotional access difficulty that gets attributed to autism as a core feature may actually belong to the alexithymia running alongside it.
For neurodivergent women in perimenopause, this isn't a new problem that menopause created. It's an existing wiring difference that the hormonal transition is exposing and amplifying. The flatness feels sudden because the buffer disappeared — but the underlying pattern was there long before the hot flashes started.
The good news in that is real: if you address the nervous system foundation — the interoceptive access, the body-first translation skills, the stress and sleep load that compounds everything — the hormonal transition becomes something your nervous system can navigate rather than something that dismantles you.

When to Escalate Clinically
If what you're reading here sounds like your daily life — the emotional flatness, the disconnection, the feeling that you're going through the motions — that pattern deserves a proper clinical look, not just a self-care plan.
I work with women at exactly this intersection: the hormonal transition, the nervous system load, the stress, gut, and sleep disruption that travels with it. I order comprehensive labs before our first meeting — not after — so we have the full picture of what your hormones, your stress response, your thyroid, and your metabolic markers are actually doing. If you're in California, Georgia, Kentucky, Maryland, Ohio, Texas, or Virginia, you can book a Reset Foundations Consult at drstaceydenise.com/reset-foundations-consult. For women outside those states, the Color Reset Series is where the TLC-SAY™ practice lives in full.
Take the Next Step
The quiz takes five minutes. It identifies your Color Archetype — how your nervous system tends to process emotional input, sensory experience, and regulation. That's your entry point into TLC-SAY™ and the work that may help bring you back to yourself.
Take the Free Color Archetype Quiz →👇🏽
Sources
Hynd M et al. Estradiol modulates resting-state connectivity in perimenopausal depression. Journal of Affective Disorders. 2024. DOI: 10.1016/j.jad.2024.11.068
Berent-Spillson A et al. Metabolic and hormone influences on emotion processing during menopause. Psychoneuroendocrinology. 2016. DOI: 10.1016/j.psyneuen.2016.08.026
Kinnaird E et al. Investigating alexithymia in autism: a systematic review and meta-analysis. European Psychiatry. 2019. DOI: 10.1016/j.eurpsy.2018.09.004
Mahler K et al. An interoception-based intervention for improving emotional regulation in children in a special education classroom: feasibility study. Occupational Therapy in Health Care. 2024. DOI: 10.1080/07380577.2024.2313527
Murphy J, Catmur C, Bird G. Alexithymia is associated with a multidomain, multidimensional failure of interoception: evidence from novel tests. Journal of Experimental Psychology: General. 2018. DOI: 10.1037/xge0000361
Dr. Stacey Denise is a board-certified surgeon transitioned into lifestyle medicine specializing in the menopause transition. She sees patients in California, Georgia, Kentucky, Maryland, Ohio, Texas, and Virginia.ge0000361
